
 (119)
(119)


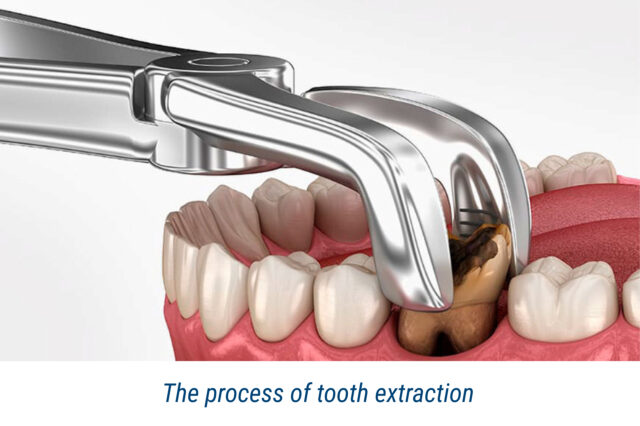
Tooth extraction is a serious surgical procedure, after which it is necessary to restore the gum and the bony socket from which the root was extracted.
To avoid complications, it is essential to follow the recommendations of the attending physician and pay attention to the slightest signs of abnormalities.
One of the likely consequences is alveolitis. Specialists of the Clinic of Aesthetic Dentistry will tell you what this pathology is, why it occurs, and how it manifests itself. We will also tell you about the methods of diagnosis and therapy.
What Is Alveolitis?
Alveolitis (another name, ‘alveolar osteitis’) – inflammation in the bone cavity from which the tooth was removed. Pathology can occur for several reasons.
Most often, it occurs due to damage to the blood clot. This is the name of the clot that forms in the hole after tooth extraction. It is needed to protect the wound from infection, getting inside saliva and food particles. In addition, blood clots are essential for tissue regeneration. A blood clot should never be removed. It will gradually dissolve itself.
If the clot has not formed or is destroyed prematurely (e.g. due to intensive gargling), bacteria will enter the alveolus. Moreover, the ‘dry hole’ syndrome can result from poor hygiene and infectious processes. In people with weak immunity, alveolitis appears due to a tendency to develop inflammation in the body.
Symptoms of Alveolitis
- Sharp pain that does not fade but, on the contrary, intensifies.
- Hyperaemia and swelling of the gum’s soft tissues at the tooth extraction site.
- Discharge of pus or other exudate from the alveolus.
- Appearance of mouth odour.
- Enlargement of lymph nodes under the jaw and sometimes in the neck.
- Fever.
Types and Stages of Alveolitis
Alveolitis can be serous, purulent and hypertrophic. The inflammatory process in all cases runs differently.

Serous alveolitis: initial stage
Signs of pathology are observed a couple of days after extracting the tooth from the hole. Distinctive features of serous alveolitis are the following:
- partial or complete absence of thrombus;
- peeking of exposed bone from the socket;
- aching, throbbing pain that increases with touch;
- swelling of the gingiva;
- formation of single pustules in the form of dots.
If untreated, the serious form of inflammation progresses to a more severe stage.
Purulent alveolitis: how to recognise it
This condition can be observed on the 5th to 7th day after surgical intervention. Pain is even more intensified and radiates to the temple, ear, and neck (along the course of the trigeminal nerve). It becomes difficult to chew and open the mouth.
A grey plaque appears in the cavity, except for the gum, the surrounding tissues around the wound swell. Submandibular and cervical lymph nodes become enlarged and painful. Hyperthermia (rise in body temperature above 37 degrees Celsius) is observed.
Chronic alveolitis: complications
This stage is called hypertrophic. Symptoms subside: pain decreases, hyperthermia passes, and general well-being improves. However, granulations form in the socket itself, and pus continues to flow out. The alveolus becomes livid.
If the disease is not treated, the purulent-necrotic process passes to the deep layers of tissues, which may result in dangerous complications:
- abscess – melting of subcutaneous fat tissue;
- osteomyelitis – damage to the jawbone;
- periostitis (flux) – inflammation of the periosteum;
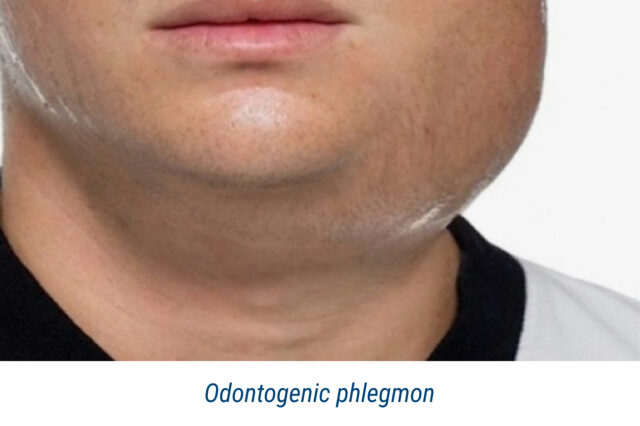
- phlegmon – infection in the subcutaneous layer of the jaw.
Diagnostic Methods
The diagnosis of ‘alveolitis’ is set by collecting the patient’s anamnesis and complaints, visual inspection and additional tests. The doctor’s task is to determine the severity and nature of the course of alveolitis to identify the factors that provoked inflammation. A dental surgeon carries out the diagnosis. If necessary, other specialists are involved.
Visual examination
On examination, it can be found that the blood clot has partially disintegrated or is not present at all. The bone tissue of the alveolus is exposed, and food residues may accumulate in the socket.
The alveolus walls are inflamed, and a dirty-grey plaque with an unpleasant odour and pus discharge is visible. The gingival mucosa is hyperaemic and swollen.
The lymph nodes in the corresponding area are more sore when palpated. The patient feels sharp pain when touching the socket.
X-rays and other ways of examination
Hardware diagnostics help to detect bone fragments, remnants of the tooth root, and purulent-necrotic processes in the bone tissue (osteomyelitis). In some situations, it may require:
- study of the exudate to determine the type of infection;
- a general blood test;
- clinical tests to assess soft tissue conditions.
Treatment of Alveolitis
The therapy of alveolar osteitis involves sanitation of the socket, rinsing with antiseptics, and using anaesthetics and antibacterial drugs. The prognosis is favourable if the patient quickly appeals to the dentist.
Reducing inflammation
Therefore, treatment begins with treating the socket. If a clot has fallen out after tooth extraction, a procedure consisting of the following steps is performed:
- Local anaesthesia.
- Cleansing of the alveolus from accumulated food, pus and necrotised tissue.
- In some cases – curettage: the removal of granulation tissue from the socket’s walls by scraping.
- Treatment with an antiseptic solution.
- Tamponade with the use of medication to accelerate healing.
Use of antiseptics
Antiseptics help eliminate bacterial infections, create a sterile environment in the hole, and control inflammation. They are also used for mouth baths, socket irrigation, and soaking tampons.

Most commonly used in alveolitis:
- Chlorhexidine – destroys most varieties of microorganisms.
- Furacilin (Nitrofurazone) – has an antiseptic and anti-inflammatory effect.
- Hydrogen peroxide – is used to clean the hole from pus and necrotised tissue.
- Iodoform – has antiseptic and antifungal properties.
Prescribing antibiotics
Antibacterial drugs destroy pathogenic microorganisms, prevent the spread of infection to nearby tissues and organs, help relieve inflammation and reduce pain.
A dentist may prescribe antibiotics in the following cases:
- Extraction of several teeth at once.
- Presence of concomitant diseases in the patient – other oral pathologies, immunodeficiency conditions, diabetes mellitus, etc.
- The risk factors – smoking and poor dental care.
Antibiotics should only be taken when prescribed by a dentist. The dosage must be precisely followed, and the duration of therapy must be observed. Even if symptoms improve and disappear, treatment must be completed; otherwise, there is a risk of infection recurrence.
Recommendations After Tooth Extraction
- First hours after the procedure:
- gauze swab, which the dentist has placed in the hole, should be kept for 20-30 minutes; this is enough time for the formation of a clot;
- to reduce pain and swelling, a cold compress (ice wrapped in a towel) can be applied to the cheek; if necessary, the procedure should be repeated after 15 minutes;
- do not eat for two to three hours (until the anaesthesia wears off);
- you can drink warm water;
- it is crucial to avoid overheating and physical activity;
- no mouthwash may be given for 24 hours.
- First days:
- food should be soft; hard, spicy and hot foods are forbidden;
- chewing should be on the opposite side;
- tooth extraction aftercare should be gentle – use a soft brush, do not touch the socket;
- if necessary, use an anaesthetic prescribed by the doctor;
- It is recommended that you sleep in a reclining posture with your head elevated for the first 24 hours. You can use two pillows.
- What you should avoid doing:
- keep the swab in your mouth for longer than half an hour;
- touch the socket with the tongue, etc.
- rinse the mouth excessively;
- go to a bath or sauna;
- make warming compresses;
- sunbathing in the sun or visiting a solarium;
- exercise;
- smoke;
- drink alcohol;
- lift heavy weights.

Timing of healing of a cavity after tooth extraction
When you should see a dentist:
- 1. Severe pain persists even after taking medication.
- Fever has increased in body temperature.
- Bleeding lasts longer than 2 hours after tooth extraction.
- Swelling persists or increases.
- Pus is oozing from the socket.
- Gum stitch removal after tooth extraction with gingival incision is required.
Each case is different, so the timing of soft tissue healing may vary. If you follow the attending physician’s instructions and adhere to a healthy lifestyle, you will not have to deal with alveolitis and other complications after anesthesia and tooth extraction.

