 (1)
(1)


Many patients with periodontitis live for years in fear of losing their teeth, believing that implants are not an option for them. In fact, modern medicine allows implants to be placed even in cases of serious gum disease. However, it is important to understand that periodontitis is an unpredictable condition.
According to a study in Clinical Oral Implants Research, people with periodontitis are 3.1 times more likely to develop inflammation around the implant than healthy people. But there is good news: if the doctor and patient follow the correct preparation protocol, implants take root and last for decades in 92-95% of cases.
At the KES clinic, we do not consider periodontitis a contraindication but rather a condition that requires specific preparation. Below, we will describe in detail the steps needed to ensure a titanium implant lasts for decades despite chronic gum disease.
Dental implants for periodontitis
Is it possible to have implants fitted if you have periodontitis?
Yes, but only when the disease is in remission. Periodontitis is an active infection. If an implant is fitted when the gums are inflamed, bacteria will attack it immediately. In medicine, this is called high adhesion (the ability to stick) of pathogens to metal surfaces: harmful microbes can colonise the surface of an implant in just 30 minutes. This is a direct path to the loss of the structure.
Conditions under which we at KES admit a patient for surgery:
- Depth of gum pockets: no more than 5 mm. If the pockets are deeper (6 mm or more), they harbor billions of bacteria, increasing the risk of implant loss by 45%.
- No bleeding: the gums should not bleed during examination. We aim for a bleeding index below 15%.
- Cleanliness: the patient must brush their teeth perfectly. If there is a lot of plaque, the risk of implant rejection increases exponentially.
Only when these three conditions are met do we begin the main stage — implant placement.
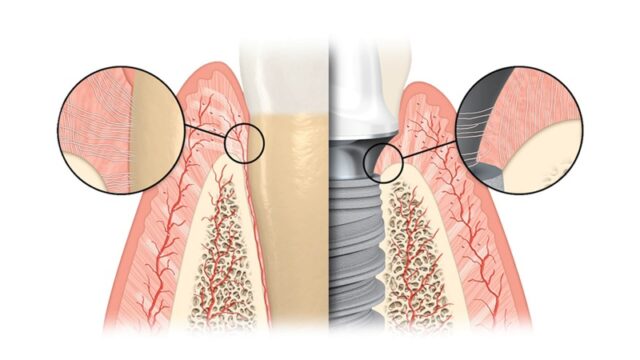
Why does periodontitis complicate the process?
The problem is not only in the gums, but also in what happens underneath them — in the bone.
Destruction of the foundation
Periodontitis causes the bone to resorb. Chronic inflammation leads to significant bone loss, making implant placement impossible without prior bone grafting. For implant placement, the bone must be sufficiently dense. The doctor assesses this using computer tomography data.
Specific immunity
Studies show that many patients with periodontitis have a genetic trait: their immune system reacts too strongly to even the slightest plaque. Where plaque causes only minor gum inflammation in a healthy person, a patient with periodontitis experiences an aggressive defensive reaction. The body perceives bacterial accumulation as a serious threat and rapidly destroys the bone around the implant, attempting to isolate itself from the source of infection.
Preparing the cavity: a step-by-step protocol
At KES, we eliminate random factors when planning treatment. Implant placement is performed only after thorough diagnosis and the creation of biological conditions that guarantee its stability and durability. Our goal is to create a sterile zone.
First, we remove teeth that cannot be saved (those that are loose and have lost more than 70% of their support). They are the main sources of infection.
Then we clean the remaining teeth. The key tool here is ultrasonic scaling. Ultrasound operates at 25–30 kHz, producing the effect of micro-explosions of water bubbles. This destroys the protective shell of bacteria and breaks up tartar in the deepest places. This treatment removes up to 90% of all mouth infections in a single session.

Ultrasonic cleaning
Preparing for surgery
- Rinsing with antiseptic mouthwash: we prescribe special rinses (0.12–0.2% chlorhexidine) 2–3 days before surgery. This significantly reduces bacterial activity in the oral cavity and prevents their spread, creating a safe environment for surgery.
- 3D diagnostics (CBCT): We assess not only bone volume but also its quality. To install a standard implant, the bone width must be at least 6–7 mm to ensure sufficient bone tissue around the implant on all sides.
- Bacteria test: In complex clinical cases, we conduct a laboratory analysis of the microbiota to accurately identify the pathogen and select the antibacterial drug to which the bacteria are most sensitive.
Implant Selection and Surgery
If you have a medical history of periodontitis, using low-cost or ‘universal’ systems carries a high risk of rejection. Dentists prefer implants with an active hydrophilic surface. This structural feature stimulates osseointegration (fusion with bone) twice as fast, ensuring reliable fixing even in conditions of reduced blood supply to tissues.
Key technical parameters:
- Primary stability (torque): for immediate loading, a torque of at least 35 N·cm is required. If primary stability is low (less than 20 N·cm), immediate loading is not used: the implant requires a 3-6 month rest period for reliable osseointegration, and only then is the crown installed.
- Special thread design: the presence of microthreads in the implant neck stabilises the bone and gum levels. This prevents tissue resorption (loss), keeping it within physiological norms — no more than 0.1–0.2 mm per year.
- Use of navigation templates: individual 3D templates allow the implant to be positioned with an accuracy of 0.1 mm. This allows the use of the densest areas of bone, minimising gum damage.

Implant placement in periodontitis
Lifelong care: how to preserve implants
Patients with periodontitis should keep in mind that implants require more rigorous care than natural teeth. Without systematic care, inflammatory complications develop in 20–25% of cases within 5 years.
- The ’90-day’ professional hygiene mode: visit the hygienist strictly every 3 months. It is during this period that pathogenic microflora manages to form stable, aggressive colonies (biofilm) capable of destroying the implant fixation.
- Mechanical hygiene (irrigator): the use of a water jet at 500–600 kPa is the only way to remove plaque under orthopaedic devices without damaging the gingival cuff.
- Safe cleaning: professional hygiene in the clinic should be carried out exclusively with low-abrasive powders (based on erythritol). The use of standard soda results in microscratches on titanium, increasing bacterial colonization by 60%.
Our Clinic of Aesthetic Dentistry has specialised in the rehabilitation of patients with complex periodontal conditions for over 25 years. Our approach is based on comprehensive tissue treatment and the creation of a reliable biological foundation for long-lasting results.

